
Diabetes Mellitus
Diabetes is a Metabolic and Chronic Disease that causes troubles and degrades the quality of life of millions of people.
Diabetes can be treated. It depends on many factors, such as the extent of biochemical aberrations, the patient’s preferences, the specialization of the Medical team, as well as the macro-environment.
Diagnosis of Real Causes & Treatment of Diabetes Mellitus
- Gradual restoration of cellular function
- Personalized therapeutic protocols, without chemical residues and excipients
- Treating the real causes
- Therapeutic formulas that work alone or in combination with any other medication
- Adopting a Molecular / Therapeutic Nutrition Plan
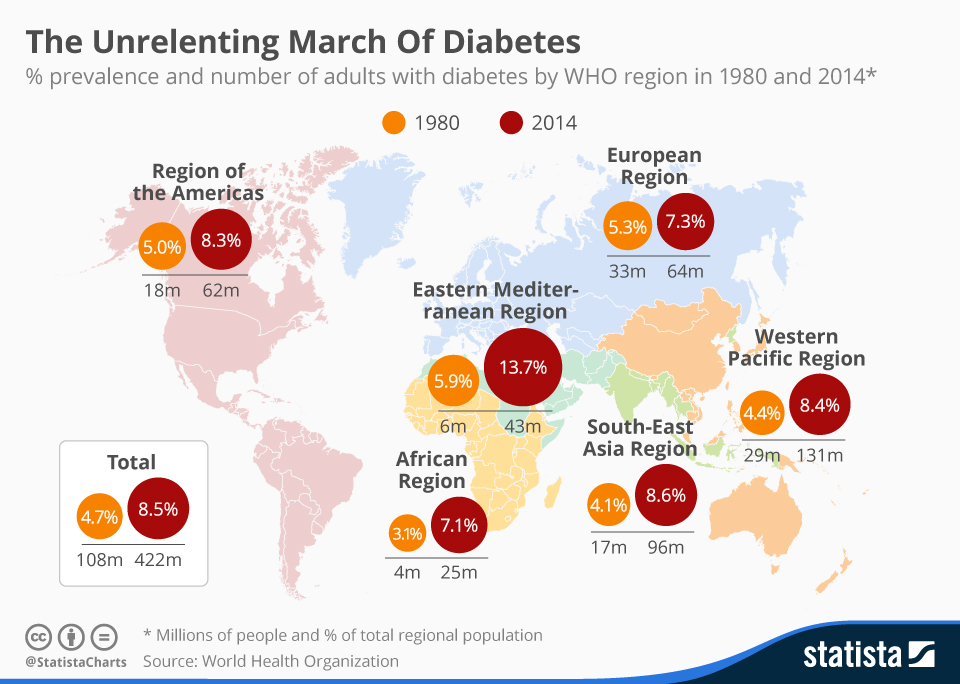
Diabetes Mellitus is one of the most common diseases worldwide with rapid growth rate.
According to the World Health Organization (WHO), more than 422,000,000 people had Diabetes until 2014. We almost reached to half a billion people in 2016.
It is estimated that by 2030 the population suffering from Diabetes Mellitus will have doubled, reaching to about one billion.
Diabetes Mellitus will be the 7 th Cause of Death worldwide, since it already leads to heart diseases, with tragic ending, Chronic Renal Failure, Amputations and Blindness.
Today in Greece, according to the official data only, on 31-5- 2016, the individuals suffering from Diabetes Mellitus were 1,187,370, exceeding 11% of the population.
Great amounts of money are spent annually on Diabetes. More than $ 350 billion in the USA and around $160 billion in Europe.
Diabetes Mellitus and Cellular Level
It is only lately, having understood and realized how biochemical composition is influenced at the cellular level, scientists and pioneering research centers can now talk about Metabolic Diseases treatment.
Our body is actually a colony of billions of cells. They take care of the organism’s Life and proper functioning. This is achieved through their ability to communicate with each other through the process of Homeostasis. Homeostasis is a process of maintaining a stable and invariant state from our cells, independently of external changes.
Continuous deviations and contrasting interventions on cellular functions, at the biochemical level, which may be accumulating for years, underlie and at some point they manifest, in the form of Disease.
Through the intervention, correction and restoration of cell’s biochemical balance we can have our good and properly functioning Health back.
Insulin resistance may be a pre-existing condition, as already mentioned, before the onset of Diabetes for many years (like in cases of Obesity or Metabolic Syndrome) and it is called Prediabetes.
It is also estimated that 20-25% of patients with Type 2 Diabetes are not diagnosed.
Actually they have Latent Autoimmune Diabetes in Adults (LADA).
These patients with diabetes are not overweight and can live healthily, but they should continue receiving insulin treatment, because of pancreatic dysfunction.
Insulin Resistance and Diabetes Mellitus affect virtually all aspects of physiology.
When sugar can’t get into a cell, it oxidizes and turns into Advanced glycation end products (AGEs) end products.
When we say that something oxidizes, think of it like rust on a car. AGEs combined with high levels of insulin are Inflammatory.
They cause destruction to tissues, such as retinas, nerves, kidneys, and blood vessels, as well as to all proteins of the body, resulting in “silent inflammations”.
“Silent inflammations” are the main cause of all Diseases and Immature Aging.
Diabetes Mellitus and Treatment
Until today, it includes dietary interventions and encouragement to increase physical activity. Patients undergo exhaustive, crash diets, while at the same time they are required to strictly follow and concentrate on their program. The results are minor, while there is great discomfort for patients. Although pharmaceutical treatments, which used to fall into two categories and now fall into six, can regulate blood glucose (sugar) levels, they are administered for life and they do not protect from other diseases that develop over time, such as: heart diseases, hypertension, etc. The administration of injectable insulin, which is also for life, is used to restore hormonal balance. The patient should take his/her daily dose so that to be functional.
Surgical operations for obesity, which may delay drug administration and reduce the years of administration while reducing the quantities of insulin. However, complications of surgical operations are serious and there is discomfort for patients.
Insulin is one of the few hormones that you have direct control over. Better management of insulin can prevent the onset of diabetes and many other Chronic Diseases.
Our body can better determine on its own what happens to it.
All these metabolic disorders can be corrected and our organism can regain its initial balance.
Treatment Protocols with Micronutrients – Regimens
Biochemical aberration at the level of organism’s functioning can be measured through the relevant biochemical or metabolic exams. There is a large number of exams and tests available according to the Medical History to ultimately determine the treatment regimen. The cost of most exams is affordable. The results are ready within two to three days.
Micronutrient protocols, according to the American Standards, strictly define the dosage, duration, quantity and combination of ingredients (formula) per person.
Depending on the extent of the lesions and the individual findings treatment may last from six to eighteen months to fully restore the patient’s clinical picture.
Treatment Protocols with Biomimetic Hormones
The wide popularity of biomimetic (bioidentical) hormones is due to the fact that they are natural, thus our body can metabolize them similarly to its own hormones, without any side effects.
Biomimetic Hormones bind (“snap”) on our hormonal receptors, exactly as the key fits into its lock, providing a direct effect, as opposed to the traditional hormone replacement therapy, where synthetic hormones are poured over hormonal receptors, but also on other steroid receptors, and finally their effect is both non direct, but also a lot of side effects may occur.
Patients see their everyday life improving gradually, together with their overall physical condition.
These therapies are systematically used in clinical practice since 1997, and the country of departure was the United States of America. They are not contradictory to any other concurrent pharmaceutical or homeopathic treatment.
The appropriate treatment is that which ultimately provides the best possible benefit, according to the clinical outcomes and the relevant exam markers.
Diabetes Mellitus – Background Information
Diabetes Mellitus is among the Metabolic Disorders, i.e. disorders that affect metabolism.
Metabolism is the process and its mechanisms, during which our body uses appropriately the foods consumed to transform them to energy. The energy our organism needs at cellular level to function.
Metabolism is substantially the transformation of energy from one form to another. Therefore, when we receive each type of food (carbohydrates, proteins, fats), the organism, through metabolism, transforms it to glucose (sugar). This glucose is the energy molecule that should enter into our cells so that they perform their activities. It is our organism’s fuel.
What is Diabetes Mellitus (Sugar Diabetes)
Everyone knows that Diabetes Mellitus is the increased concentration of glucose (sugar) in the blood. This is the final result, what is actually happening, i.e. Hyperglycemia.
Diabetes Mellitus and Nutrition
Hyperglycemia occurs because the glucose (sugar) circulating in the blood cannot enter into our cells and be utilized.
To achieve this, Insulin in essential. Insulin is a hormone, which is produced by specific pancreatic cells, B-cells. They are located in clusters within a special area of the pancreas, called islets of Langerhans.
Insulin is the “vehicle” and the “key” to transfer but also to put inside the cells glucose circulating in our blood.
So, Diabetes Mellitus occurs:
- Either because Β-cells of the pancreas do not produce (secrete) sufficient quantity of Insulin,
- or because our body cannot use effectively the produced insulin (Insulin Resistance),
- or because both the above are present.
Glucose (sugar) circulates in the blood and its levels increase constantly, while at the same time cells do not receive the required energy to perform their functions.
Diabetes Mellitus – Types
There are three main types of Diabetes Mellitus:
Type I Diabetes Mellitus
Λέγεται και Ινσουλινοεξαρτώμενος Σακχαρώδης Διαβήτης ή Νεανικός Σακχαρώδης Διαβήτης ή J.O.D. (Juvenile Onset Diabetes).
Στην περίπτωση αυτή, έχουμε καταστροφή των Β-κυττάρων του παγκρέατος. Αποτέλεσμα να μην παράγεται καθόλου ινσουλίνη (ολική έλλειψη) ή να έχουμε ελάχιστη έκκρισή της. Το πάγκρεας είναι κατεστραμμένο είτε λόγω Αυτοανοσίας (δυσλειτουργία ανοσοποιητικού), είτε λόγω κάποιου ιού. Πρόκειται για Χρόνιο Νόσημα.
Ο Σακχαρώδης Διαβήτης τύπου 1 , αποτελεί την κυριότερη μορφή διαβήτη στα παιδιά, μπορεί ωστόσο να προσβάλλει και ενήλικες. Η Νόσος παραμένει δια βίου.
Type I Diabetes Mellitus
Also called Insulin-Dependent Diabetes Mellitus ή or Juvenile Onset Diabetes Mellitus (J.O.D.).
In this case, damage of the pancreatic B-cells occurs. As a result, either no insulin is produced (total deficiency), or its secretion is minimal. The pancreas is damaged either due to Autoimmunity (dysfunctional immune system), or due to a virus. It is a Chronic Disease.
Type 1 Diabetes Mellitus is the main type of Diabetes among children, but it can also occur in adults. The Disease is present for life.
Type 2 Diabetes Mellitus
Also called Non-Insulin Dependent Diabetes Mellitus.
In this type of Diabetes, there is either insufficient insulin produced by the pancreatic B-cells, or insulin produced does not respond adequately to its purpose, due to the resistance of our body’s organs and tissues (Insulin Resistance).
Circulating glucose (sugar) increases, since it cannot enter into cells effectively.
Type 2 Diabetes Mellitus accounts for about 90% of all cases of Diabetes.
This is also a Chronic Disease. Both genes, but mainly acquired, external factors are responsible, such as diet, lifestyle, improper sleeping, toxicosis (toxic load), and multiple micro-nutrients deficiencies.
Gestational Diabetes Mellitus
This type of Diabetes occurs sometimes (3-5%) during pregnancy.
It affects women, who never had Diabetes Mellitus before pregnancy. It is similar to Type 2 Diabetes Mellitus.
It occurs during this period, due to the great changes of the pregnant woman’s metabolism, and hormones. The mechanism of secretion of normal levels of Insulin from pancreatic B-cells is “blocked” from the intense action of Placental hormones. The organism, in an attempt to balance insulin deficiency, triggers pancreatic B-cells to produce up to the double quantities of Insulin.
However, sometimes this is not achieved, resulting in the appearance of Diabetes Mellitus.
Gestational Diabetes Mellitus occurs mainly in overweight women at the beginning of pregnancy, in cases of family history, as well as in women above 35 years of age.
Gestational Diabetes Mellitus is a reversible Disease. It usually resolves after childbirth. Nevertheless, it is extremely dangerous throughout pregnancy. It causes severe perinatal complications (preeclampsia, eclampsia pregnancy, hypertension), and it may even be life-threatening for the mother and fetus. The babies of mothers who are overweight or had Gestational Diabetes Mellitus have increased risk in their life to be Overweigh, have Impaired Glucose Tolerance (IGT), and Diabetes Mellitus (30-40%).
Diabetes Mellitus – Manifestations and Symptoms

Diabetes Mellitus is an insidious disease. Often no symptom is present. Patients may ignore that they have it for years.
The onset of Type 1 Diabetes Mellitus is usually sudden and fulminant, and the main symptom is the occurrence of a dangerous condition, called Diabetic Ketoacidosis (DKA). It is potentially life threatening and it presents suddenly, with nausea and vomiting, abdominal pain, tachypnea, flushing, hyperglycemia (blood glucose level above 240 mg/dL), polyuria and loss of consciousness (fainting episode).
Type 2 Diabetes Mellitus, which is the most common type, usually occurs with the following symptoms:
Polydipsia (excessive thirst), Polyuria and frequent urination especially at night (nocturia), Binging and increased hunger, Weight loss, which is due to cells’ inability to uptake glucose, Visual problems, such as turbidity, Pruritus (itching sensation in the body), Intense fatigue, permanently, Recurrent fungal vaginitis in women and other genital infections, Delayed wound healing and minor injuries, Frequent Inflammations and Infections, Dry and cold Skin, Dry mucous membranes, Peripheral Neuropathy.
Prediabetes
Before the presentation of Type 2 Diabetes Mellitus, a condition called Prediabetes occurs. This condition may be underlying for years.
During this phase, the levels of glucose may be higher than normal limits, but not high enough to help in disease diagnosis.
In particular fasting glucose (sugar) value (IFG – Impaired Fasting Glucose) ranges from 100 to 125 mg/dl, while when post-meal sugar or the Oral Glucose Tolerance Test (OGTT) is between 140 and 199 mg/dl, then the patient has Prediabetes.
Moreover, patients who have Prediabetes have also developed Insulin Resistance.
The sooner Prediabetes is identified, the better the chances, through the right treatment, that the patient will not develop Type 2 Diabetes.
Type 2 Diabetes Mellitus – Causes
Diabetes Mellitus, as mentioned above, is a Metabolic Disease. At the same time, it becomes a Chronic Disease for most patients worldwide.
There is no permanent cure, while together with Diabetes, many concurrent diseases usually also occur, making patients suffer more.
The causes are multiple according to the literature.
They mainly focus on lifestyle, nutrition and hereditary factors. However, there are many studies and surveys, the data of which are contradictory or not mutually supportive.
Type 2 Diabetes Mellitus and Heredity
In the case of heredity, we should understand that many genes have been implicated. More than 36 different genes contribute in the increased possibility for this disease to occur among people who have these. They are usually involved in pancreatic B-cells dysfunctions.
Nevertheless, the genes are only increasing the predisposition of a person, they do not inherit the disease itself. Furthermore, the rate relating to the family history of Diabetes among sufferers is only 40%, while the total number of genes involved in this disease constitutes only 10% of hereditary factors involved in Diabetes.
Type 2 Diabetes Mellitus and Obesity
In the case of Obesity, accumulated fat is implicated. Fat, no matter where it is (subcutaneous, visceral, organic fat) presents Insulin Resistance.
This Resistance means that tissues’ cells cannot use effectively Insulin, the levels of which are initially normal. The first tissues showing Insulin Resistance are the Liver, the Muscles, and the Adipose tissue.
Our organism, to cope with this urgent situation, triggers the pancreas and B- cells secrete more and more Insulin. Insulin’s action in the Liver is to inhibit (stop) glucose release in the blood. However, due to Liver’s Insulin Resistance, the Liver constantly releases more glucose in the blood. As a result of this, circulating Glucose (sugar) increases continuously. Firstly because of the constantly increasing release of new Glucose from the Liver, and secondly due to cells’ inability to let it enter inside them, due to the existing Insulin Resistance.
Metabolism is deviating. It is totally disorganized.
Type 2 Diabetes Mellitus and Pathophysiology
The pancreas, in its attempt to cope with these extreme, stressful conditions, starts wearing out. Its initially permanent Overactivity to produce Insulin, leads to fatigue and subactivity. And finally Insulin production is inadequate, resulting in the gradual increase of blood Glucose (sugar).

Type 2 Diabetes Mellitus and Correlations
We know that Obesity is another Metabolic Disease. It is caused by the consumption of large quantities of foods that are rich in calories but not in nutrients.
Moreover, we know that poorly processed carbohydrates, which also share these characteristics, are stored by our body in the form of fat.
The overall imbalance of the organism occurs when our body moves away from what is normal. The above mentioned type of diet, lack of fibers, large (one or two) and infrequent (five to seven) meals, starchy snacks, lack of exercise, stress, and smoking, lead our body to produce increasingly larger quantities of hormones in order to balance this.
In the case of Diabetes Mellitus, Insulin. However, imbalance of one hormone in the human body leads to imbalance of the Hormonal System as a whole.
Diabetes Mellitus and Metabolic Diseases

It is also easily understood that all Metabolic Diseases are inextricably interrelated to each other. They may come and go or develop simultaneously. They manifest at the same time or at different times, having the same main causes, which are never dysfunctions of the organs initially.
Polycystic Ovary Syndrome (P.C.O. Syndrome) is another characteristic example, as it is another cause triggering Diabetes Mellitus. At least 40% of women suffering from this Syndrome also manifest Diabetes Mellitus before the age of 40 years old.
And here is the common philosophical question: “Which came first: the chicken or the egg?”. Since Syndromes trigger Chronic Diseases. And Chronic Diseases cause other Chronic Diseases and Syndromes. In a vicious cycle.
What actually documents the resounding failure in treating all Chronic Diseases, including Diabetes Mellitus, is that patients have to follow crash diets, exercise and pharmaceutical treatments for life, and they are never cured. They never are or feel Healthy.
The 8 aspects of your health that are impacted by Insulin in detail:
- Insulin tells your liver to make more cholesterol. Cholesterol is the precursor to many of our hormones, including cortisol. Our body produces more Cholesterol in response to the demands placed on it. This is a highly intelligent response to your environment and lifestyle, not an error. Your body never makes mistakes.
- Insulin increases Blood Pressure by increasing sodium retention. Many diabetics also have high blood pressure (Blood Hypertension), as a result of insulin issues.
- Insulin keeps your liver in a state that is able to detoxify properly. The liver is like your body’s oil filter. The liver takes the trash and sludge out of your blood, but it can’t do as good of a job when insulin and blood sugar are constantly elevated.
- Insulin promotes Inflammation, the very thing that causes Insulin Resistance. Inflammation promotes joint pain, cardiovascular disease, fluid retention, and weight gain to name a few. These diseases are often seen in patients with Diabetes Mellitus.
- High insulin levels in women cause them to make more Testosterone. Symptoms include the polycystic ovarian syndrome (PCOS), with hair thinning, and unwanted face and body hair. Insulin can also affect the distribution of weight, causing weight gain in the mid section of the body.
- Men, due to Insulin, produce higher levels of Estrogens. This can contribute to breast enlargement (gynecomastia) and prostate problems among men. At the same time, they also manifest erectile dysfunction and reduced of libido (sexual motivation).
- High levels of insulin are also directly related to higher risk for colon Cancer and breast Cancer. Insulin promotes cellular division and thus it accelerates cancer cell division. Cancer is more common in patients with Diabetes Mellitus.
- High levels of Insulin promote weight-gain because it is a fat storage hormone. When insulin can no longer drive sugar into cells so that to produce energy, its next job is to store that sugar and fat for use at a later time. But this is something that never happens!
It becomes clear the amount of devastation that can be caused by a single hormone. However, imbalance of one hormone in the human system leads to imbalance in the Hormonal System as a whole.
All these disturbances lead to Obesity, Cardiovascular Diseases, Hypertension, Immature Aging, Metabolic Syndrome, Depression, and Cancer.
Dr. Nikoleta Koini, M.D.
Doctor of Functional, Preventive, Anti-ageing and Restorative Medicine.
Diplomate and Board Certified in Anti-aging, Preventive, Functional and Regenerative Medicine from A4M (American Academy in Antiaging Medicine).
References:
- Global report on diabetes. World Health Organization, Geneva, 2016.
- Projections of global mortality and burden of disease from 2002 to 2030. Mathers CD, Loncar D. PLoS Med, 2006, 3(11):e442.
- Markesbery, W. Damage to Lipids, Proteins, DNA, and RNA in Mild Cognitive Impairment. Arch Neurol. 64(7):954-956; July, 2007.
- Mecocci, P., et al. Arch Neurol 59:794-798; May, 2002.
- Geroldi, C., et al. The InCHIANTI Study. Arch Neurol 62; July, 2005:, 1067-72.
- Ohara; T., et al. Glucose tolerance status and risk of dementia in the community, The Hisayama Study. Neurology September 20, 2011 vol. 77 no. 12 1126-1134.
- Ott, A., et al. Diabetes mellitus and the risk of dementia, The Rotterdam Study. Neurology 53:1937-42, December, 1999.
- Yaffe. MD, et al. Advanced glycation and product level, diabetes, and accelerated cognitive aging. Neurology October 4, 2011 77:1351-56.
- Enzinger, C., et al. Annual brain volume change. Neurology 64:1704-11; May 24, 2005.
- Wild RA. Obesity, lipids, cardiovascular risk and androgen excess. Am J Med 1995;98:27S-32S.
- Zakrzewska KE, et al. Glucocorticoids as counterregulatory hormones of leptin: toward an understanding of leptin resistance. Diabetes 1997;46:717-719.
- Zakrzewska, et al. Induction of obesity and hyperleptinemia by central glucocorticoid infusion in the rat. Diabetes 1999;48:365-370.
- Bermeis K, Vosmeer S, Kelly U. Effects of glucocorticoids and of growtu hormone on serum leptin concentratons in man. Eur J Endocrinol 1996;663-665.
- Weiderpass E, et al. Diabetes mellitus and risk of large bowel cancer. J Natl Cancer Inst 1997;89:660-661.
- Brenner R. Nutrition and hormonal factors influencing desaturation of essential fatty acids. Prog Lipid Res 1982;20;41-48.
- Matejkova-Behanova M. Latent autoimmune diabetes in adults (LADA) and autoimmune thyroiditis. Endocr Regul. 2001 Sep;35(3):167-172.
- Unnikrishnan AG, Singh SK, Sanjeevi CB. Prevalence of GAD65 antibodies in leansubjects with type 2 diabetes. Ann N Y Acad Sci. 2004 Dec;1037:118-121.
- Appel SJ, Wadas TM, Rosenthal RS, Ovalle F. Latent autoimmune diabetes of adulthood (LADA): an often misdiagnosed type of diabetes mellitus. J Am Acad Nurse Pract. 2009 Mar;21(3)156-159.
- Nambam B, Aggarwal S, Jain A. Latent autoimmune diabetes in adults: A distinct but heterogeneous clinical entity. World J Diabetes. 2010 Sep 15;1(4)111-115.
- Zhou J, Ma XJ, BaoYQ, Pan XP, Lu W, Hu C, Xiang KS, Jia Wp. [Study on prevalence of latent autoimmune diabetes in adults and its relationship with metabolic syndrome]. Zhonghua Yi Xue Za Zhi. 2009 May 12;89(18):1250-4.
- Zhonghua, Yi Xue Za Zhi. 2009 May 12;89(18):1250-1254.
- Brooks-Worrell B, Palmer JP. Immunology in the Clinic Review Series; focus on metabolic diseases: development of islet autoimmune disease in type 2 diabetes patients: potential sequelae of chronic inflammation. Clin Exp Immunol. 2012 Jan;167(1):40-6.
- Li X, Zhou ZG, Yang L, Huang G, Yan X. [Metabolic syndrome and latent autoimmune diabetes in adults]. Zhongguo Yi Xue Yuan Xue Bao. 2003 Dec;25(6)676-9.
- Schernthaner G, Hink S, Kopp HP, Muzyka B, Streit G, Krosis A. Progress in the characterization of slowly progressive autoimmune diabetes in adult patients (LADA or type 1.5 diabetes). Exp Clin Endocrinol Diabetes. 2001;109 Suppl 2:S94-108.